Where Is the Ureteropelvic (UP) Junction?
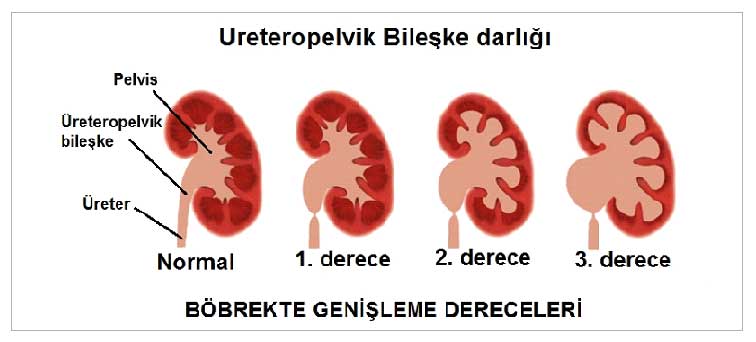
Urine produced by the kidneys is first collected in a reservoir called the renal pelvis and then transported to the bladder via tube-like structures called ureters. The point where the renal pelvis meets the ureters is called the ureteropelvic junction. A narrowing that develops at this point is defined as ureteropelvic junction obstruction.
The ureteropelvic junction is the site where obstruction (narrowing) is most commonly observed in the upper urinary tract. UP obstruction is present in as many as 64% of children born with hydronephrosis (kidney enlargement).
For urine produced in the kidneys to pass from the renal pelvis into the ureter, a structurally sound ureteropelvic junction is required. In addition, the rhythmic contractions of the ureter—known as peristalsis—also aid in this transport. Both of these components must be structurally sound to ensure proper urine flow. Problems at the ureteropelvic junction can be intrinsic to the ureter itself or extrinsic in origin. Narrowing of that section of the ureter is the most common cause. In addition, there may be extrinsic problems, such as abnormally positioned blood vessels.