Ureteral Stricture
What Is Ureteral Stricture?
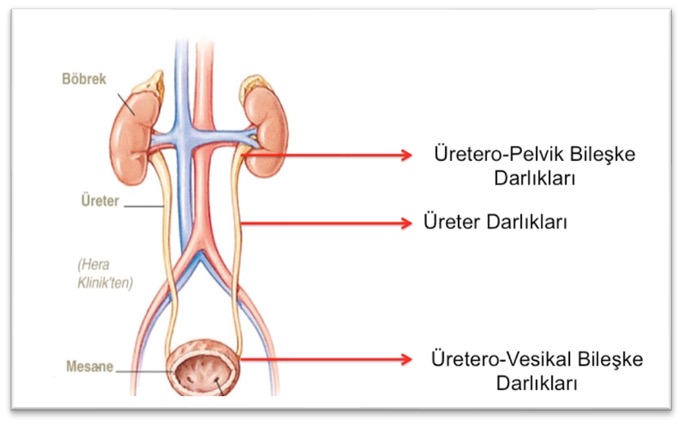
Ureteral stricture is a narrowing or blockage that occurs in any part of the ureter, the tube that carries urine from the kidneys to the bladder. The ureter’s normal function is to safely and efficiently transport urine from the kidneys to the bladder. Ureteral stricture can obstruct the flow of urine and lead to back pressure in the kidneys (hydronephrosis), which can cause kidney damage. This condition can lead to complications such as pain, urinary tract infections, bleeding, or loss of kidney function.
What are the causes of ureteral stricture?
Ureteral strictures can develop due to various factors. These causes are generally related to congenital or acquired conditions.
- Congenital Causes:
- Ureteropelvic Junction Stenosis (UPJ Stenosis): This is a narrowing that occurs at the point where the ureter joins the kidney (the ureteropelvic junction) and is usually congenital. This condition can block the flow of urine from the kidney into the ureter, leading to fluid buildup (hydronephrosis). UPJ stenosis is the most common cause of congenital ureteral narrowing.
- Ureteral Atresias: A portion of the ureter may be congenitally blocked or underdeveloped, which obstructs the flow of urine.
- Traumatic Causes:
- Pelvic Trauma: Accidents, falls, or surgical procedures in the pelvic region can lead to injury and narrowing of the ureter. Pelvic fractures or major surgeries (such as gynecological or urological surgeries) can cause damage to the ureter.
- Laparoscopic and Robotic Surgeries: Procedures performed during robotic or minimally invasive surgeries can cause injury to the ureter. There is a risk of damaging the ureter, particularly during pelvic and abdominal surgeries.
- Inflammation and Infections:
- Chronic Infections: Chronic urinary tract infections, particularly kidney infections, can lead to the formation of scar tissue in the ureter and, as a result, narrowing of the ureter.
- Tuberculosis: Renal tuberculosis is an infection that affects the ureter and can cause narrowing. It often affects other organs as well.
- Cancer and Tumors:
- Ureter Cancer: Cancers that develop in the ureter itself or in nearby organs can cause narrowing of the ureter. As the cancer grows, it can lead to a blockage of the urinary tract.
- Pelvic Cancers: Cancers in the areas through which the ureter passes can spread to surrounding tissues, causing narrowing of the ureter. In women in particular, surgical treatments for uterine and cervical cancer can lead to ureteral stricture.
- Kidney Stones:
- Kidney Stones: Kidney stones or ureteral stones can narrow the ureter by causing prolonged obstruction. This condition can lead to inflammation and scar tissue formation in the tissues surrounding the stone’s location.
- Post-Stone Scarring: Microtraumas that occur during stone treatment or as the stone passes can narrow the ureter and, over time, lead to an obstruction.
- Postoperative Scarring:
- Urological and Abdominal Surgeries: Pelvic surgeries—particularly urological cancer surgeries, kidney transplants, or postpartum complications—can damage the structure of the ureter and lead to its narrowing. Additionally, ureteral narrowing may occur following anterior urethral surgery.
What are the symptoms of ureteral stricture?:
The symptoms of ureteral stricture vary depending on the severity of the narrowing and the location of the stricture. The following symptoms are commonly observed:
- Due to the narrowing, the flow of urine from the kidney to the bladder is blocked, and pressure builds up in the kidneys. This can cause back pain or flank pain.
- Fluid buildup in the kidney can lead to swelling and enlargement (hydronephrosis).
- Urinary Tract Infections
- Blood in the urine (hematuria)
- Difficulty Urinating: The bladder cannot empty completely, and as a result of urine retention, you may experience frequent urination, a sense of urgency, or difficulty urinating.
- If the narrowing is left untreated for a long time, it can lead to permanent damage to kidney function.
What methods are used to diagnose ureteral stricture?:
Ureteral stricture is diagnosed based on the patient’s symptoms, a physical examination, and various imaging methods.
- Physical Examination and Medical History
- Ultrasonography
- Intravenous Pyelography (IVP)
- Computed Tomography (CT) and MRI Pyelography: CT or MRI imaging techniques can be used to examine narrowing of the ureter in greater detail. These methods are particularly useful for examining the pelvic region.
- Retrograde Ureteropyelography (RUG): This is another specialized imaging method used to detect narrowing in the ureter.
- Endoscopic Evaluation (Cystoscopy and Urethroscopy): Endoscopic techniques are used to directly visualize the ureter. This is very helpful in determining the location and severity of strictures in the urethra.
- Urinalysis: Symptoms of infection and kidney function can be monitored. Blood and protein tests can be used to detect kidney damage or infection.
How is ureteral stricture treated?
Treatment for ureteral stricture varies depending on the severity, location, and cause of the stricture. Treatment options include:
- Conservative Administration:
- Follow-up: If a stenosis does not cause any specific symptoms, regular follow-up and monitoring may be recommended. A watch-and-wait approach may be used, particularly for small stenoses that do not cause obstruction.
- Endoscopic Procedures:
- Balloon Dilatation: A balloon catheter is inserted into the area of the narrowing to widen it. This procedure is typically used for mild and temporary narrowings.
- Stent Placement: A stent may be placed to temporarily dilate the ureter and ensure urine flow. This method is typically used until a decision is made regarding surgical intervention.
- Surgical Treatment:
- Ureteroplasty: The narrowed portion of the ureter is removed and repaired using grafts taken from surrounding tissues (oral mucosa, skin, or tissues surrounding the kidney).
- Ureteral Anastomosis: The narrowed section is removed, and the healthy ends of the ureter are sutured together.
- Ureteral Reconstruction: If there is a severe stricture, a long segment of the ureter can be removed and reattached to the remaining healthy tissue.
- Minimally Invasive Surgical Techniques (Laparoscopic and Robotic Surgery): Laparoscopic or robotic surgery is less invasive than traditional open surgery, and patients recover more quickly.
What are the advantages of laparoscopic and robotic surgery in the treatment of ureteral strictures?
These techniques are used particularly in cases requiring reconstruction following ureteropelvic junction (UPJ) obstruction, ureteral stricture, ureteral injury, and cancer.
The Advantages of Laparoscopic and Robotic Surgery
Because laparoscopic and robotic surgeries are minimally invasive techniques, they offer many advantages over traditional open surgery:
✅ Smaller Incisions: This results in less tissue damage and smaller scars.
✅ Faster Recovery: Patients are discharged sooner than with open surgery.
✅ Less Blood Loss: Blood loss is much lower with minimally invasive techniques.
✅ Less Pain: Thanks to the small incisions, the patient experiences less postoperative pain.
✅ Faster Return to Daily Life: The time it takes to return to work and social life is shorter.
✅ Lower Risk of Complications: The risk of infection, incisional hernia, and tissue damage is low.
✅ Better Cosmetic Results: Because the incisions are small, patients are left with minimal scarring.
Robotic surgery takes the advantages of laparoscopic surgery a step further. By providing three-dimensional (3D) visualization, more precise suturing techniques, and improved ergonomics, it allows the surgeon to perform the procedure with greater control.
In What Situations Is Laparoscopic or Robotic Surgery Used?
Laparoscopic and robotic surgery are preferred, particularly in the following situations:
- a) Ureteropelvic Junction (UPJ) Obstruction
- The most common condition is congenital ureteral stricture.
- Urine flow is blocked at the point where the ureter joins the kidney (the ureteropelvic junction).
- b) Ureteral Strictures (Narrowing of the Ureter Due to Scarring)
- It can develop as a result of trauma, kidney stones, infections, or surgery.
- c) Surgical Repair of the Ureter (Ureteral Reconstruction)
- Ureteral damage may occur following pelvic surgery or radiation therapy.
- d) Ureteral Tumors and Post-Cancer Reconstruction
- In cases of ureteral cancer or tumors that have spread to surrounding organs, it may be necessary to remove part of the ureter.
What is the difference between laparoscopic and robotic surgical techniques?
The main techniques used in minimally invasive ureteral surgery, whether performed laparoscopically or robotically, are as follows:
- A) Laparoscopic Pyeloplasty (Used for Ureteropelvic Junction (UPJ) Stenosis)
- This is the surgical correction of a narrowing between the kidney and the ureter (UPJ obstruction).
- Method: The narrowed section of the ureter is removed, and the remaining healthy tissues are anastomosed (reconnected).
- Success rate: Around 90–95%.
- B) Robotic Pyeloplasty
- It is the robot-assisted version of the laparoscopic procedure.
- Robotic surgery may yield better results, particularly in cases of complex strictures or following previous unsuccessful surgeries.
- C) Laparoscopic Ureteroplasty
- In cases of ureteral strictures, the narrowed segment is removed and the ends of the ureter are sutured together.
- Advantage: The recovery time is much shorter compared to open surgery.
- D) Robotic Ureteroplasty
- It is preferred because of its advantages of precise suturing and minimal blood loss.
- Tissue grafts (oral mucosa, intestinal segments) can be used in wide or long strictures.
- E) Laparoscopic Boari Flap Surgery (for Lower Ureteral Strictures)
- A portion of the bladder is used in place of the ureter to reconstruct the ureter.
- Indication: This procedure is preferred when a large portion of the ureter is damaged.
- F) Laparoscopic or Robotic Ureteral Implantation (Reimplantation)
- It involves reattaching the ureter to the bladder.
- Indications: Used in the treatment of lower ureteral strictures or vesicoureteral reflux.
How Does Da Vinci Robotic Surgery Differ from Traditional Methods?
Da Vinci robotic surgery offers significant differences compared to traditional surgical methods:
Fewer Cuts:
While traditional surgery involves larger incisions, Da Vinci robotic surgery uses minimally invasive techniques to make much smaller incisions. This speeds up the recovery process and reduces the risk of infection.
3D Imaging:
The Da Vinci system provides the surgeon with high-resolution 3D and magnified images. This allows the surgeon to see the surgical site in greater detail. With traditional methods, however, the surgeon’s view is more limited.
Precision and Control:
The arms of robotic surgery systems have much greater precision and flexibility of movement compared to the human wrist. This allows the surgeon to reach more difficult-to-access areas and perform more precise procedures. In traditional surgery, this level of precision and flexibility is more limited.
Less Pain and Faster Recovery:
Because of the smaller incisions, patients experience less postoperative pain and recover more quickly. In traditional surgery, however, the recovery process may take longer due to the larger incisions.
Less Blood Loss:
Because robotic surgery allows for more precise manipulation of tissues, there is less blood loss during surgery. The rate of blood loss is generally higher with traditional methods.
Surgeon's Comfort:
The Da Vinci system allows the surgeon to perform the surgery from a seated console. In traditional surgery, the surgeon must stand for long periods, which can lead to fatigue and loss of concentration.
These differences make Da Vinci robotic surgery a safer, more effective, and more comfortable option in many cases.
What should we be mindful of after ureteral stricture surgery?
- Length of Hospital Stay: Patients undergoing laparoscopic or robotic surgery can be discharged within 1–3 days.
- Recovery Time: It is much shorter than with open surgery; most patients can return to their normal lives within 1–2 weeks.
- Pain: Minimal; mild pain relievers are usually sufficient.
- Urinary Catheter: A urinary catheter may be used for 5–7 days.
- Stent Use: A DJ stent is temporarily placed while the ureter heals; this stent is removed after 4–6 weeks.
- Follow-up: Follow-up examinations are performed within the first 3–6 months using ultrasound, kidney function tests, and, if necessary, CT or MRI urography.
Conclusion
Laparoscopic and robotic surgery are considered among the best options for treating ureteral strictures. Compared to open surgery, they offer a lower risk of complications, faster recovery, and better cosmetic outcomes. Robotic surgery allows for more precise and successful outcomes, particularly in complex cases.
Conclusion and Follow-up:
Ureteral strictures can be treated, but patients must be monitored regularly after treatment. The success rate of treatment varies depending on factors such as the type, location, and severity of the stricture. During follow-up, urine flow is monitored regularly, infections are prevented, and additional surgical interventions may be performed as needed to address recurrent strictures.
Send Your Message