Artificial Bladder
- What Is an Artificial Bladder (Neobladder)?
- In What Situations Do We Use an Artificial Bladder?
- Is an Artificial Bladder Suitable for Every Patient?
- Who Should Not Have an Artificial Bladder Implanted?
- Is There an Alternative to an Artificial Bladder?
- What Should the Preparation Process for an Artificial Bladder Be Like?
- How Does an Artificial Bladder Work?
- What Should You Keep in Mind During the Postoperative Recovery Process?
- What Should We Keep in Mind in the Long Term When Using an Artificial Bladder?
- What Kinds of Complications Can Occur with an Artificial Bladder?
- Will I Be Able to Urinate Normally After an Artificial Bladder?
- Conclusion
What Is an Artificial Bladder(Neobladder)?
An artificial bladder is a new urinary bladder created using the body’s own tissue when the natural bladder must be removed due to various health issues. It is typically used in cases such as bladder cancer. This surgical procedure is performed to improve the individual’s quality of life and help them maintain natural urinary function as much as possible.
In What Situations Do We Use an Artificial Bladder?
- Bladder Cancer: This is the most common reason for bladder removal. In this surgical procedure, the natural bladder is removed and an artificial bladder is created.
- Neural Tubes: Problems related to the nervous system, such as spinal cord injuries, can affect urinary function. In such cases, an artificial bladder may be a solution.
- Chronic Bladder Disorders: In some chronic conditions that cause a loss of bladder capacity or significantly impair bladder function, a bladder replacement may be necessary.
Is an Artificial Bladder Suitable for Every Patient?
An artificial bladder (neobladder) is not a suitable option for every patient. This procedure depends on many factors, such as the patient’s overall health, surgical eligibility, and lifestyle.
Patients Suitable for an Artificial Bladder;
People in Good General Health
- People who do not have serious systemic diseases such as heart, lung, or kidney disease.
Patients Who Can Undergo Urethral Preservation
- If the urethra is not affected by cancer and can be safely preserved, an artificial bladder may be implanted.
Those with Suitable Intestinal Conditions
- It may not be suitable for patients with a history of serious intestinal diseases (Crohn's disease, ulcerative colitis, etc.).
Patients Who Can Learn to Urinate
- Since an artificial bladder does not function like a natural bladder—which relies on muscles and nerves—the patient must learn how to urinate.
- It is suitable for patients who are able to empty their bladder by using their abdominal muscles.
Who Should Not Have an Artificial Bladder Implanted?
People in Poor General Health
- Patients with heart failure, severe lung disease, or advanced kidney failure
People Who Need to Have Their Urethra Removed
- If cancer has spread to the urethra or if the urethra must be removed due to a tumor, a urinary diversion cannot be performed.
People with Intestinal Diseases
- It is risky for patients with inflammatory bowel diseases (Crohn's disease, ulcerative colitis, etc.) because their intestinal tissue is not suitable.
Patients Who Will Be Unable to Learn to Urinate or Control Their Urination
- Patients with neurological disorders (spinal cord injury, MS, etc.) may be unable to control their urination.
- Elderly patients or those with impaired cognitive function may also be unable to manage this process.
This procedure is technically relatively simple and reliable, and is therefore the most commonly used form of diversion.
When choosing this type of urinary diversion, you should be aware that you will need to invest time and effort to adjust to living with a stoma. Your healthcare team will help you adapt your lifestyle and get used to the situation (changes in your body’s appearance, sports and hobbies, travel, etc.).
Is There an Alternative to an Artificial Bladder?
If an artificial bladder is not an option, other methods of urinary diversion may be considered:
- Ileal Conduit: The drainage of urine through a stoma (an opening in the abdominal wall).
- Continual Urostomy (Indiana Pouch): An internal urine reservoir that is drained via a catheter.
In conclusion, an artificial bladder may not be suitable for every patient and should be evaluated on a case-by-case basis. Would you like me to conduct a specific evaluation for you or a patient?
What Should the Preparation Process for an Artificial Bladder Be Like?
Diagnosis and Evaluation:
Doctors may perform ultrasounds, cystoscopies, MRIs, and CT scans to evaluate the condition of the urinary tract.
Consulting:
Psychological and physical counseling provides patients with information about the pros and cons of surgery, the recovery process, and life after surgery.
Dietary Changes:
Before surgery, patients are asked to stop consuming alcohol and tobacco and to prepare by following a generally light diet.
How Does an Artificial Bladder Work?
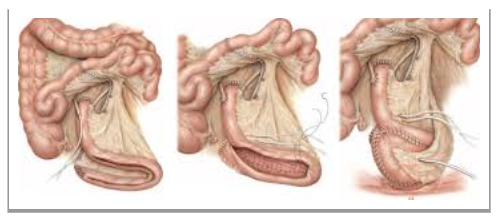
A 40-60 cm section of the small intestine (ileum) is removed to be used as a bladder substitute. The remaining sections of the intestine are reconnected to the digestive system. The removed intestinal segment is flattened and then folded into a sphere or a U-shape to form a pouch capable of holding urine.
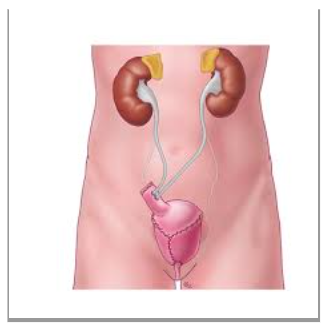
The ureters (urinary tracts) are connected to the artificial bladder, allowing urine to flow from the kidneys to this new storage site. When the artificial bladder (neobladder) is connected to the urethra, the patient can urinate naturally by using their muscles. However, some patients may experience incontinence or difficulty emptying their bladder.
What Should You Keep in Mind During the Postoperative Recovery Process?
Initial Recovery Period:
Observation: The first few days are spent in the intensive care unit or in a hospital ward under constant observation.
Catheter Use: The urinary tract can be drained externally using a catheter until the new bladder has fully healed.
Pain Management: Postoperative pain is managed with pain relievers prescribed by a doctor.
Active Recovery:
It is important to adjust your diet and fluid intake. Adequate fluid intake helps the urinary tract function properly.
Gradual physical rehabilitation
Bladder training: This teaches the bladder how to signal when it is full and how to use the muscles effectively to gain control.
What Should We Keep in Mind in the Long Term Regarding an Artificial Bladder?
- Regular Medical Checkups: Regular visits to the doctor are necessary to monitor healthy functioning and detect potential problems early.
- Dietary Recommendations: Since it may affect kidney function, a diet low in protein and sodium may be recommended.
- Activity Level: Regular, light exercise is recommended to maintain fitness and keep the intestines healthy.
- Psychological Support
- Physical therapy and, if necessary, catheterization may be used to treat functional problems such as urinary incontinence or difficulty urinating.
What Kinds of Complications Can Occur with an Artificial Bladder?
Because artificial bladder (neobladder) surgery is a major surgical procedure, it can lead to various complications in both the short and long term.
- Early-Stage (First Weeks After Surgery) Complications
a) Surgical Complications
- Bleeding:
- Anastomotic Leak (Urine Leak): Urine may leak from the points where the artificial bladder is connected to the ureters or the urethra. This is usually managed with drainage, but in severe cases, repeat surgery may be necessary.
- Bowel Problems: A bowel obstruction (ileus) may develop, and if it does not resolve within a few days, surgery may be necessary. Leakage may occur at the surgical incision sites, which can lead to serious infections.
b) Infections
- Medium- and Long-Term Complications
a) Functional Problems
- Urinary Incontinence:
- Daytime bladder control usually develops within a few months, but some patients may experience nighttime accidents.
- Kegel exercises are recommended to strengthen the pelvic floor muscles.
- Difficulty Urinating:
- Since the artificial bladder is not controlled by nerves, the patient must learn to urinate by using their abdominal muscles.
- Some patients may need to undergo catheterization (urinary drainage using a catheter) because they are unable to fully empty their bladder.
b) Metabolic Problems
- Metabolic Acidosis:
- When a segment of the intestine comes into contact with urine, bicarbonate is lost, and an acidic environment may develop in the body.
- It can cause symptoms such as fatigue and shortness of breath. It can be corrected with sodium bicarbonate supplementation.
- Renal Dysfunction:
- Over time, the backflow of urine into the kidneys (vesicoureteral reflux) can impair kidney function. c) Accumulation of Stones and Mucus
- Stone Formation in an Artificial Bladder:
- Since it is made from intestinal tissue, stones may form inside the artificial bladder.
- Drinking plenty of water and urinating regularly can help prevent this.
- Mucus Production:
- Because the intestinal segment is still producing mucus, mucus may accumulate in the bladder.
- You may need to urinate regularly and, at times, flush out your bladder.
- Rare but Serious Complications
- Fistula Formation: Abnormal connections may develop between the artificial bladder and the intestine, skin, or vagina.
- Artificial Bladder Stricture: A narrowing may occur at the urethral junction, which can make urination difficult. Dilation or surgery may be necessary.
- Cancer Risk: There is a small risk of cancer developing in the bladder from intestinal tissue many years later. Regular follow-up is essential.
Will I Be Able to Urinate Normally After an Artificial Bladder?
With an artificial bladder, patients can largely return to their normal lives. However, since the new bladder lacks nerve connections, patients typically urinate by contracting their abdominal muscles. Some patients may need to use a catheter to empty their bladder and may experience problems such as infections or stones. They may also need training on how to control and empty their bladder.
Conclusion
Artificial bladder surgeries require a detailed evaluation due to their complexity and potential risks; however, with modern medical technology and ongoing treatment protocols, they provide a significant improvement in patients’ quality of life after surgery. The medical team recommends that patients attend a detailed preoperative information session, during which the benefits, potential risks, and possible outcomes of the surgery are carefully explained. A personalized treatment plan should be developed based on each patient’s individual needs and life goals.
Send Your Message