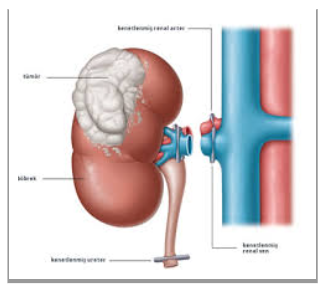
What Is a Kidney Tumor?
Kidney tumors can originate from the functional tissue of the kidney (renal parenchyma) or the collecting system (urothelium). Most are malignant and typically grow without causing symptoms, often being detected incidentally. The most common type of kidney cancer is renal cell carcinoma (RCC), which accounts for approximately 85–90% of kidney tumors.
Kidney cancer is being diagnosed at an earlier stage more frequently, particularly with the widespread adoption of advanced imaging techniques in recent years. As a result, treatment options have expanded, and minimally invasive surgical techniques have come to the forefront.
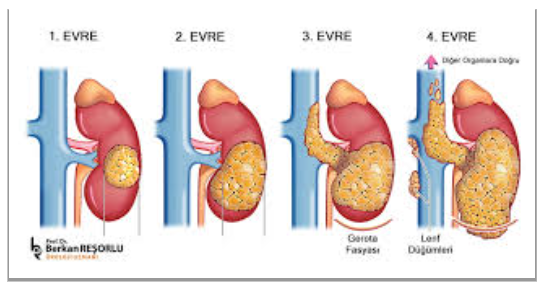
Early-Stage (Localized) Kidney Cancerni (T1-T2) How Do We Treat It?
- Surgical treatment (nephrectomy or partial nephrectomy)
- T1a (<4 cm) tümörlerde böbrek koruyucu cerrahi (parsiyelnefrektomi) tercih edilir.
Locally Advanced (T3-T4) and Metastatic Disease?
- Surgery + Systemic Therapy (Immunotherapy and Targeted Therapies)
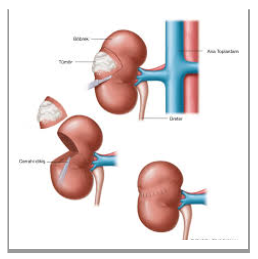
Can the Cancer Be Removed from a Kidney Tumor While Preserving the Kidney Itself?
Yes, in cases of kidney tumors, it is possible to remove only the cancerous tissue while preserving healthy kidney tissue. This procedure is called a partial nephrectomy (kidney-sparing surgery) and is the preferred method, particularly for small and medium-sized kidney tumors (stages T1a–T1b).