Why Is the Importance of Testicular Cancers Increasing?

Testicular cancers are more common, particularly in high-income countries.
Among solid tumors—what we refer to as mass tumors—treatment success rates remain high even in cases of metastatic disease (spread to other sites).
Complete remission is possible in 85–90% of patients. However, because these tumors have the potential to spread rapidly, surgery and treatment are required as soon as possible.
What Are the Reasons for Seeking Treatment for Testicular Cancers?
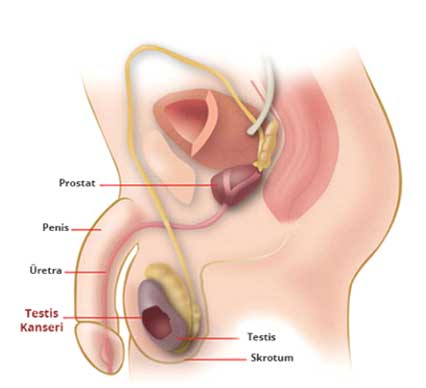
 Patients typically present with painless swelling and a mass (hardness) on one side. Twenty percent of patients present with scrotal pain (pain in the scrotum—the skin and subcutaneous tissue covering the testicles).
Patients typically present with painless swelling and a mass (hardness) on one side. Twenty percent of patients present with scrotal pain (pain in the scrotum—the skin and subcutaneous tissue covering the testicles).
Unless proven otherwise, painless scrotal induration should be considered a testicular tumor—unless there is a history of inflammatory conditions—and managed accordingly.
Back and flank pain occur in 11% of cases; in addition, rare symptoms such as hemoptysis (coughing up blood), nausea, vomiting, convulsions (seizures), and bone fractures may occur in 10–20% of cases due to metastatic masses. Gynecomastia (enlarged breasts) may occur in 7% of patients.