What Is the Bladder and What Does It Do?
The bladder—the medical term for the urinary bladder—is an important organ located in the urinary tract of our body. The primary and basic function of the bladder is to store urine from the kidneys and to ensure that this urine is voluntarily emptied at appropriate intervals—that is, to urinate.
How Is Bladder Cancer Classified?
Bladder cancer is classified histologically and clinically:
A) Histological Classification (Type of Cancer)
1. Urothelial Carcinoma (Transitional Cell Carcinoma) → This is the most common type (90%).
2. Squamous Cell Carcinoma → Develops as a result of chronic infection or prolonged irritation.
3. Adenocarcinoma → Originates in the glandular structures of the bladder; it is rare.
4. Small Cell Carcinoma → It is quite aggressive and rare.
5. Sarcomatoid Cancer → It originates in connective tissue; it is rare but aggressive.
6. Variant Types
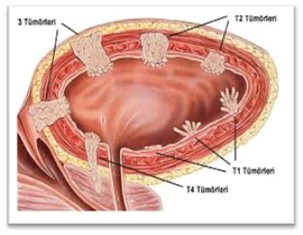
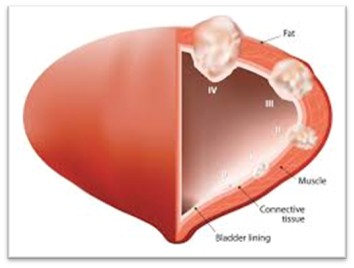
B) Clinical Classification (Depth and Spread of Cancer)
1. Superficial Bladder Cancer (Non-invasive, Ta–T1 stages) → Remains confined to the inner surface of the bladder (urothelium).
2. Invasive Bladder Cancer (Stage T2 and higher) → Has spread to the muscle layer of the bladder or beyond.
3. Metastatic Bladder Cancer → The cancer has spread to the lymph nodes or to distant organs.
How Do We Diagnose Bladder Cancer?
A) Laboratory Tests
Urinalysis → Tests for hematuria (presence of blood) and infection.
Urine Cytology → The presence of cancer cells is assessed.
Tumor Markers → Tests such as NMP22 and BTA may be helpful.
B) Imaging Methods
Ultrasonography (USG) → Useful for large tumors, but cannot detect small lesions.
Magnetic Resonance Imaging (MRI) or Computed Tomography (CT) Urography → Shows tumor spread.
Positron Emission Tomography (PET-CT) → Used to assess distant metastases.
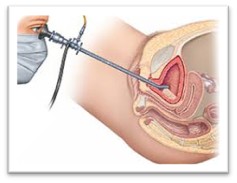
C) Endoscopic Diagnosis: Cystoscopy
Cystoscopy → The inside of the bladder is examined directly, and biopsies are taken from suspicious lesions. It is the gold standard for diagnosis.
Muscle Invasive (T2 and Higher) Bladder How Do We Treat Bladder Cancer?
1) Radical Cystectomy (Complete Removal of the Bladder)
It is the standard treatment method.
The bladder, the surrounding lymph nodes, and, if necessary, adjacent organs are removed.
- In men: The prostate and seminal vesicles may also be removed.
- In women: The uterus and ovaries may also be removed.
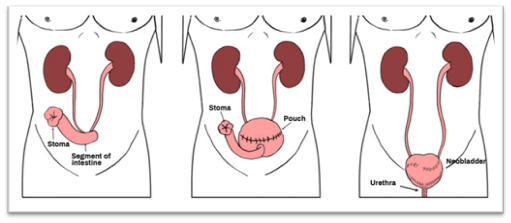
New pathways are formed to direct the flow of urine:
- Ileal Conduit: Urine is diverted to the skin using a section of the intestine.
- Orthotopic Neobladder: A new bladder is created from a section of the intestine, allowing the patient to urinate normally.
- Cutaneous Ureterostomy: The ureters are brought out directly through the skin.
2) Chemotherapy and Radiation Therapy
- Neoadjuvant Chemotherapy (Preoperative) → Administered to shrink the tumor.
- Adjuvant Chemotherapy (Postoperative) → Administered to patients with lymph node metastases.
- Radiation Therapy → It can be used for patients who are not candidates for surgery or as an organ-preserving treatment.
3) Immunotherapy and Targeted Therapies
- Checkpoint Inhibitors (Atezolizumab, Pembrolizumab) → These are new-generation treatments that activate the immune system.
- FGFR Inhibitors → Used in patients with FGFR3 mutations.