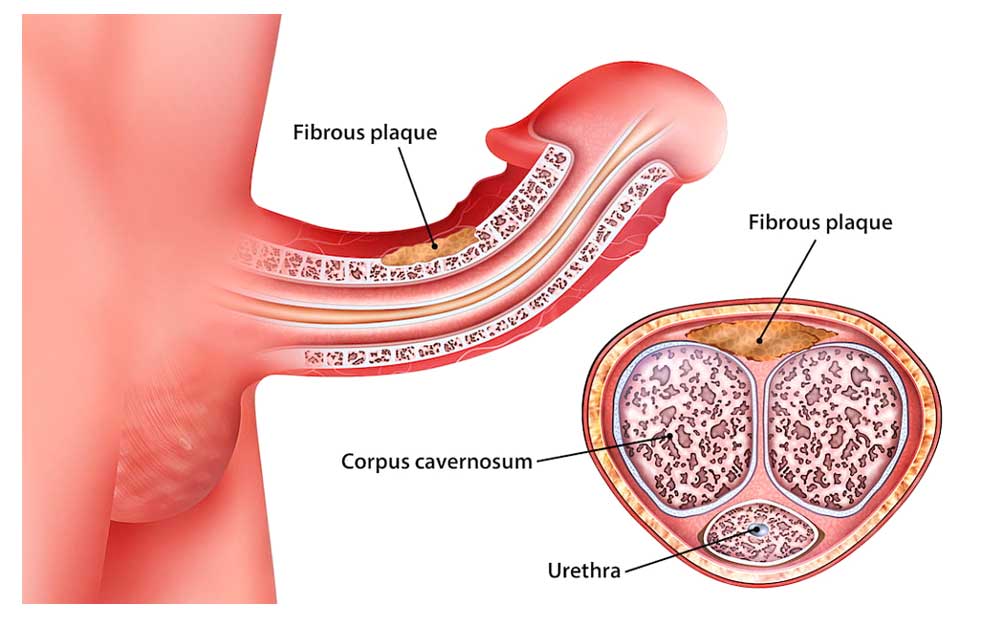
What is Peyronie’s Disease?
Peyronie’s disease is the loss of flexibility of some areas in the inner sheath of the penis that expands and grows during erection. It is also known as penile calcification.
What are the Treatment Methods for Peyronie’s Disease?
Some drugs such as Potaba or vitamin E, colchicine, tamoxifen, corticosteroids, procarbazine, orgatein, NSAIDs, seldane and allegra can provide around 30-40% improvement in the first period of the disease.
Topical treatments; corticosteroids, verapamil cream, beta-aminopropionitrile can be used. However, the success of these treatments is controversial.
Injection of verapamil, interferon, collagenase, cortisone, parathyroid hormone, and prostacyclin into the lesion may be applied.
ESWL (extracorporeal shock wave therapy): Although the mechanism of action is not known for sure, it causes direct damage to the plaque, leading to vascularization and cavitation resorption. The most common side effects are skin hematoma, hemorrhage and bleeding from the urinary tract. Surgical treatment should be preferred in cases such as penile curvature being over 40 degrees, presence of intense calcification in the plaque and the patient’s desire for rapid and effective treatment.
If the penis does not become hard enough and there is difficulty in entering the vagina, it should be corrected with surgery. If these are normal, surgery is not required.
 In cases where the curvature is mild and there are no erection problems, nesbit or plication surgeries should be performed. In cases where the curvature is severe and there are no erection problems, the patch method is used. In cases where the curvature is severe and there are also erection problems, Penile Prosthesis surgery is performed.
In cases where the curvature is mild and there are no erection problems, nesbit or plication surgeries should be performed. In cases where the curvature is severe and there are no erection problems, the patch method is used. In cases where the curvature is severe and there are also erection problems, Penile Prosthesis surgery is performed.